“You take the blue pill, the story ends, you wake up in your bed and believe whatever you want to believe. You take the red pill, you stay in Wonderland, and I show you how deep the rabbit hole goes.” – Morpheus
Take that red pill and you can never go back. In our case taking the red pill in regards to disc bulges means finding out the back pain rabbit hole goes a whole lot deeper than you ever imagined. In my series of articles you will learn what the world is really made up of. You will see some professions that treat your back pain are just snake oil salesmen in white coats. They won’t want you to understand your problem for fear they will lose money and they will lose your family and relatives that they told you to bring to them. They will put up your x-rays and tell you all that is wrong with you, but after taking the red pill you will see through them, those agents of the back pain matrix. I’m trying to free your mind. But I can only show you the door. You’re the one that has to walk through it. Education (the red pill) will set you free.
Having received a tsunami of mail regarding the athlete who I treated successfully that competed with a significant disc injury, I’ll do my best to help guide you through the disc bulge minefield. The biggest problem with low back problems, and disc problems in particular, is that most medical and paramedical professionals (let alone the local fish slapper) have never had enough education within their various undergraduate degrees to truly understand disc problems. It is a specialist’s area. Don’t let that scare you off, though. I don’t mean you cannot understand it. I mean it takes study and experience with patients to gain a depth of skill when dealing with afflicted people. Not afraid of a little hard work are we?
If you want to be a great trainer or you have a back problem and you want to understand it, here is the best place to start. I have to teach you anatomy. Understand this beast and study its habits before you engage it in battle. After the anatomy, I’ll teach you function, simple physics, and how to understand symptomatic and non-symptomatic disc problems. I’ll show you the “traffic light” system for safe exercise progression, and a whole lot more. I also figure that is going to take a lot of words, so get ready for this to be part one.
Let’s be clear. I love language. Language is specific. Words have nuances that can change whole meanings and this especially applies to scientific language. So the biggest irritant I get is when people who are not experts try to write articles on subjects that are specific and can be complex, such as disc injuries, and then totally fuck up the terminology.
In their paper Nomenclature and Classification of Lumbar Disc Pathology, doctors Fardon and Milette spent twenty pages on the clarification of the types of injuries that can occur to a disc. Dude, they never once used the term slipped. So, don’t you use it either, unless you happen use it when you say to someone who has just used the term slipped disc, “Sorry, my open hand just slipped against the side of your head rather forcefully, you idiot.”
Print out the sentence below and paste it to your favorite family photograph:
The definition of a diagnosis does not determine the symptoms.
Dammit, I think I’m going to put it on t-shirts and sell it. A specific diagnosis is a part of management consideration, but it does not dictate the treatment. Complete understanding of the nature of the symptoms and a definitive diagnosis of the problem are part of the paradigm I use to treat each individual. So, contrary to many recipe approaches, when you have a diagnosis that is specific, it does not dictate what the treatment must be. That involves a bit more understanding that will follow. For today, let’s just get our language clear and precise. I will give you a case in point later.
Here are the accepted terms you may see on a report describing the state of the disc:
- Normal – Okay, it is normal
- Congenital – Condition present at birth
- Developmental variation – Due to abnormal growth of the spine (e.g. scoliosis)
- Degenerative – A progressive impairment that can include desiccation, fibrosis, disc space narrowing, osteophytes
- Traumatic – Due to trauma
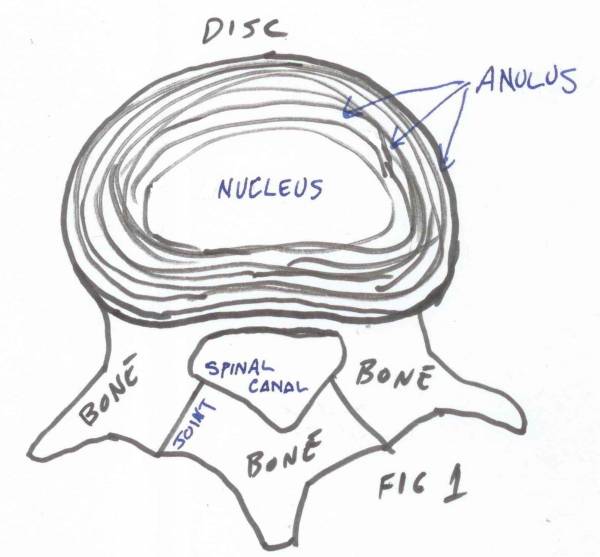 So let us look at a disc. Yes, another original drawing by me. This perspective is looking down upon a disc/vertebral section. A disc has two components you need to understand at this point. Further anatomy may be used in other articles where necessary, but today I am instructing about common disc injury terminology:
So let us look at a disc. Yes, another original drawing by me. This perspective is looking down upon a disc/vertebral section. A disc has two components you need to understand at this point. Further anatomy may be used in other articles where necessary, but today I am instructing about common disc injury terminology:
- Nucleus – in the center
- Anulus – series of rings that contain the nucleus in the middle.
What are the injuries common to a disc? Well, here we get onto more specific terminology.
- Anular tear or anular fissure – These are separations of the fibers that surround the inner part of the disc.
- Herniation – A localized displacement of disc material beyond the limits of the normal disc space. The material displaced may also be mentioned – it may be nucleus, cartilage, bone, or anular material. Herniations are subcategorized as focal, broad-based, symmetrical, or asymmetrical.
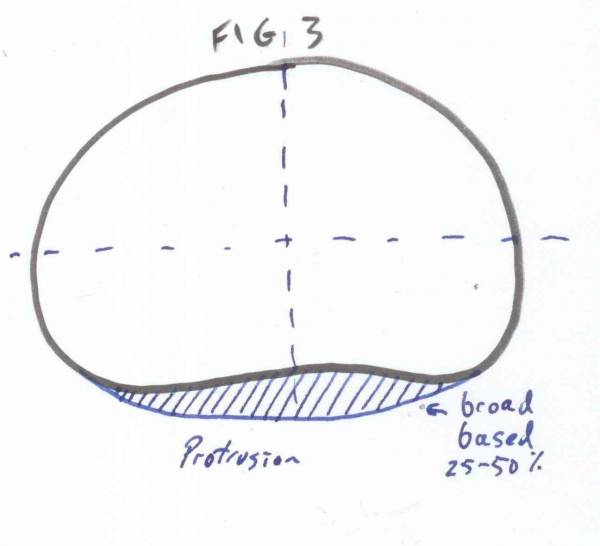
- Protrusion – A form of herniation defined by the distance it has displaced.
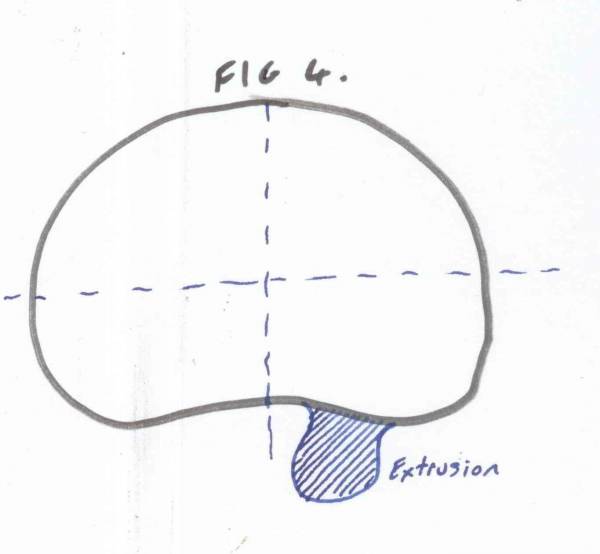
- Extrusion – A form of herniation greater than protrusion.
- Sequestration – Where the disc material has separated from the disc.
- Migration – Defines the movement of the disc material and its direction.
- Bulge – By definition this is not a herniation. It describes a generalized extension of the disc material beyond the normal disc definition. Bulging is often a normal situation requiring no treatment.
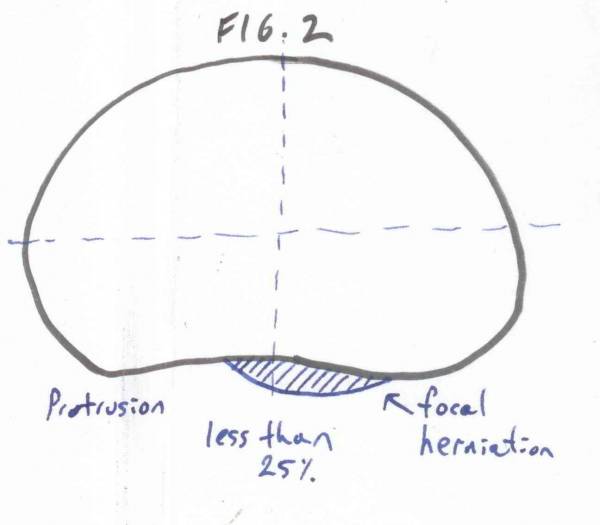 Here are some examples to help clarify the above terms. Figures 2-4 give you an idea of what I have defined. I have simply taken the disc shape and shown you how the various situations look on a CT or MRI scan. I could draw a few more but this should do for a start. (Commission art is upon request.)
Here are some examples to help clarify the above terms. Figures 2-4 give you an idea of what I have defined. I have simply taken the disc shape and shown you how the various situations look on a CT or MRI scan. I could draw a few more but this should do for a start. (Commission art is upon request.)
 So how many people do you know, or have met, who seem to consider a disc bulge as some sort of life sentence without parole? You may not have known it, but some disc bulges are absolutely normal and do not require any treatment. In fact, the person will have never felt pain or experienced impeded movement. Yet, tell someone they have disc bulge and watch how fast they press the panic button. At this time, just become more familiar with the terms and comfortable with their use.
So how many people do you know, or have met, who seem to consider a disc bulge as some sort of life sentence without parole? You may not have known it, but some disc bulges are absolutely normal and do not require any treatment. In fact, the person will have never felt pain or experienced impeded movement. Yet, tell someone they have disc bulge and watch how fast they press the panic button. At this time, just become more familiar with the terms and comfortable with their use.
 You should also become far more critical of articles written by people telling you how to treat a disc bulge or low back pain. Also there are a lot of articles published about non-specific low back pain. This to me is a term used for academic laziness. Besides radiological terminology, there is also symptomatic terminology. Any article about non-specific low back pain to me indicates the researchers were not experienced in clinical spinal rehabilitation and were unsure about how to define low back problems.
You should also become far more critical of articles written by people telling you how to treat a disc bulge or low back pain. Also there are a lot of articles published about non-specific low back pain. This to me is a term used for academic laziness. Besides radiological terminology, there is also symptomatic terminology. Any article about non-specific low back pain to me indicates the researchers were not experienced in clinical spinal rehabilitation and were unsure about how to define low back problems.
So now you know the names of the most common radiological terms for disc investigations. Now, for the bad news – a lot of doctors do not use the terminology correctly themselves. You might get an MRI scan that a radiologist will term incorrectly. Sorry, not my fault. It is up to you to be interested and to ask questions if you have a scan or are training a client with scans. Ask to look at them. It does not mean you will understand them, but the more familiar you become with them the better you will grow as a professional over the years.
So grasshopper, want to try and take that pebble from my hand yet?
The Dark Side
A “doctor” I once worked with told me he ordered MRI scans for every patient. He said the more precise the investigations you ordered the more chance you would find something wrong with the patient. That was why he did it. He knew the patient didn’t understand the amount of false positive results you can get on an MRI, but he always knew he could find something. He would make disc space narrowing appear to be a terminal condition to a frightened patient. Then he would tell the patient to bring in the husband or wife so he could explain how serious it was to the spouse as well. These people exist, they prey on you being uninformed.
References:
1. Fardon and Milette SPINE 26(5) E93-E113. Nomenclature and classification of lumbar disc pathology.
Photo courtesy of Shutterstock.
Drawings courtesy of Andrew Lock.